Stop the Sidelining Pain: Your Insider’s Guide to Tackling Piriformis & IT Band Injuries
- Abel Sanchez
- Nov 26, 2025
- 7 min read

Updated: Nov 26, 2025
You know the feeling. You’ve been pushing yourself — maybe it was that new running route on the trails just outside Eagle Pass, or the early-morning group fitness class at WYNOT that felt tougher than usual. You’ve foam-rolled until your leg is numb, you’ve stretched until you sweat,
but the ache still comes back, sinking its teeth deep into your hip or stabbing just above the knee. It’s frustrating. It’s confusing. And you’re probably asking: Why me?
Here’s the hard truth: The symptoms linked to piriformis and IT band injuries are some of the most frustrating, chronic, and sidelining pains in the fitness world. They stop you from doing what you love and make even simple daily tasks—climbing stairs, getting out of the truck, stepping off the curb after a hike—feel like a Herculean effort.
But this isn’t a textbook-definition piece. This is a practical, research-backed guide designed for people who are tired of generic advice and want to understand the why behind their pain, and more importantly, the how of true, long-term recovery.

Here’s the hard truth: The symptoms linked to piriformis and IT band injuries are some of the most frustrating, chronic, and sidelining pains in the fitness world. They stop you from doing what you love and make even simple daily tasks—climbing stairs, getting out of the truck, stepping off the curb after a hike—feel like a Herculean effort.
But this isn’t a textbook-definition piece. This is a practical, research-backed guide designed for people who are tired of generic advice and want to understand the why behind their pain, and more importantly, the how of true, long-term recovery.
1. The Dynamic Duo of Dysfunction: Piriformis and IT Band
Before we talk about fixing the pain, we need to properly introduce the culprits. These two structures — one a small, deep muscle, the other a massive sheet of connective tissue — are the pain magnates of the lower body.
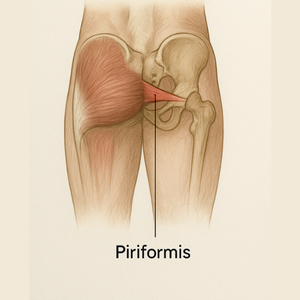
The Piriformis: The Fussy Gate-Keeper
The piriformis is that small, deep hip-rotator muscle located in your buttock, right behind your large gluteus maximus. Its job? External hip rotation. But its claim to fame (or infamy) is its location: it acts like a fussy gate-keeper for your sciatic nerve, which (for most people) runs right underneath it—but for about 15% of the population the nerve actually pierces through the muscle
itself!
When this little muscle gets tight, short, or goes into spasm—often due to overuse or, ironically, under-use—it can clamp down on the sciatic nerve. That leads to the deep, nagging ache you feel in your buttock, often radiating down the back of your leg.



The IT Band: The Super-Tough Bungee Cord
The iliotibial (IT) band is a thick, dense strip of fascia that runs from the top of your hip (where it attaches to the TFL and gluteal muscles) all the way down the outside of your thigh and attaches just below the knee. Think of it as a super-tough, non-stretchy bungee cord. Because it’s so dense and fibrous (type I collagen), its job is stability—not flexibility.
When people talk about needing to “stretch their IT band,” they are often misguided. The true problem is usually not that the band is too short, but the muscles pulling on it are weak or unbalanced—leading to friction and compression, especially at the knee.
2. The Injury Breakdown: Causes, Symptoms, and Who’s at Risk
Understanding the specifics of piriformis and IT band injuries is the first step toward effective treatment. While the pain can feel similar (hip pain, buttock ache), the underlying mechanisms are different—and so should your recovery strategy.
A. Piriformis Syndrome (The Deep Ache)
What it is: A clinical condition where the sciatic nerve is entrapped or irritated by an abnormally tight or spasming piriformis muscle.
Symptoms: A deep, nagging ache in the buttock (often worse when sitting or crossing your legs). Sometimes you feel tingling or mild radiation down the back of the thigh—but rarely past the knee. Pain worsens after prolonged sitting (yes, your office truck seat counts) or during activities that involve external hip rotation.
Who’s at Risk: Anyone whose hip mechanics are compromised. Maybe your glutes are weak, maybe your hip flexors are over-tight, or maybe you have that anatomical oddity where the nerve pierces the muscle itself.
Diagnostic Nuance: Don’t be surprised if your doctor wants an MRI or X-ray first. They aren’tignoring you—they are trying to rule out the more common suspects (like a lumbar discherniation) before pinning the blame on that fussy piriformis. In fact, piriformis syndrome is often a diagnosis of exclusion.
B. IT Band Friction Syndrome (ITBS) (The Sharp Knee Pain)
What it is: The most common cause of lateral knee pain in runners and cyclists. The pain is caused by the constant friction—or more accurately, compression—of the IT band over the lateral femoral epicondyle (that bony knob on the outside of your knee).
Symptoms: A sharp, burning pain on the outside of the knee, typically starting after a consistent period of running or cycling (for example: exactly 10 minutes into every run). It often subsides with rest but returns immediately when you resume.
Who’s at Risk: Runners (especially those increasing mileage too quickly or running hills), cyclists (up to 24% are affected), and individuals with poor core or hip stability.
Biomechanical Truth: ITBS isn’t really a “stretch” problem—it’s a strength and movement-pattern problem. Moderate evidence shows it's strongly associated with greater hip adduction and knee internal rotation during foot strike—in plain English, your hip collapses inward under load.
3. Breaking the Cycle: Effective Recovery Strategies
Okay, so now you know what it is. Time to talk about how you fix it. True piriformis syndrome recovery and ITBS relief requires a nuanced approach that addresses the root cause: weakness and poor mechanics, not just tightness.
A. When to Stretch vs. When to Strengthen (The Crucial Paradox)
This is the most critical distinction that generic advice often misses.
• Piriformis: Immediate relief comes from gentle short-hold stretches or targeted release(e.g., lacrosse ball). Long-term fix: strengthen the surrounding gluteal musculature(Gluteus Maximus & Medius) so the piriformis is not forced to over-work.
• IT Band: Foam-rolling the TFL/Glutes can help in the moment—but brutal long holds on the IT band itself are mostly a waste. The long-term fix: strengthen the hip abductors(primarily Gluteus Medius) to stabilize the hip and prevent inward collapse (which causes friction).
B. The “Magic Bullet” Tool You Need
If you only choose one tool for the piriformis? Make it a lacrosse ball or hard tennis ball.
How to use it: Sit on the floor. Place the ball under the tender spot in your buttock (that belly of the piriformis). Cross the leg (figure-four) so the foot of the working leg is over the opposite knee. Lean onto the ball and hold for 30–60 seconds, moving slightly until you find a point of high but tolerable pain. This is trigger-point therapy, fascinatingly effective for that deep muscle
spasm.
Why it works: It switches the muscle out of its hyper-spastic state, reduces nerve irritation, and gives you some immediate relief—then you immediately move into strengthening.
C. Movement Is Medicine: Gentle Exercises that Don’t Aggravate
Once the acute pain subsides, immediate introduction of gentle glute-strengthening is key.
• Clamshell: Lie on your side, knees bent, feet together. Keeping your feet touching, lift your top knee toward the ceiling. Isolates the Gluteus Medius. 3 sets Å~ 15 reps.
• Bridge (Glute Squeeze): Lie on your back, knees bent, feet flat. Push hips upward by squeezing glutes, but no lower-back hyper-extension. This fires the Gluteus Maximus, which supports the piriformis.
• Single-Leg Deadlift (body-weight or light kettlebell): Builds hip hinge pattern and forces glute activation while balancing.
Real clinical win: One study found that after a 6-week rehab program targeting gluteus medius strength and hip abductor training, 22 out of 24 injured runners were pain-free and fully back to running.
4. Preventing the Relapse: Long-Term Solutions
Here’s where most people drop the ball. You get some relief, you think you’re “fixed” — and boom: a week later you’re back to square one. The difference between “fixed” and “relapse” isn’t more rolling—it’s smarter training.
A. Core Stability Is the Foundation
Your deepest abdominal and back muscles (transverse abdominus, multifidus, obliques) keep your pelvis level when you walk, run or climb the rugged hills around the Eagle Pass area. If your core is weak, the pelvis tilts and rotates excessively—forcing your hip abductors to constantly struggle, which in turn stresses both the IT band and piriformis.
Long-term Fix: Include planks, side-planks, bird-dogs, anti-rotation work (cable or band chops) into your weekly sessions. It’s not glamorous—but it works.
B. The Local Terrain Challenge: Training Smarter
Living in an area like Eagle Pass / South Texas presents unique stresses that constantly aggravate these injuries:
• Uneven pavements and trails force your hip stabilizers (Gluteus Medius) to work harder eccentrically to prevent your pelvis from dropping. If they’re weak—the IT band tightens, the piriformis spasms.
• Sudden temperature swings (from heat to chilly morning) make your muscles stiff and less forgiving. A minimal warm-up on a crisp morning can invite a piriformis spasm.
The key: Adopt a program that anticipates these stresses rather than just reacting to them.
5. Frequently Asked Questions (FAQ)
Q: Can a tight piriformis muscle cause my knee pain?
A: Indirectly, yes. A tight piriformis can affect your gait and hip mechanics, leading to overuse and poor tracking of the kneecap. That altered mechanics stresses the IT band, and that can cause the sharp, lateral knee pain associated with IT band friction syndrome.
Q: How long does it take for piriformis syndrome recovery?
A: Mild, acute cases often improve within 2-3 weeks with rest and gentle stretching. However, chronic or severe cases—especially those rooted in deep hip weakness—can take 6-12 weeks of dedicated physical therapy and targeted strengthening to fully resolve and prevent recurrence.
Q: Should I stretch my IT band?
A: Since the IT band is dense fascial tissue, stretching it is often ineffective. The long-term fix is hip abductor strengthening (Gluteus Medius). Focus on temporarily relieving tension by stretching the muscles attached to it (glutes, TFL) and using tools like foam-rollers—but devote your recovery time to strength work.
Final Thoughts
Here’s what you need to remember: This isn’t about chasing the next shiny mobility gadget or copying someone else’s “one-size-fits-all” routine. It’s about understanding your body, adapting to your environment (yes, those Eagle Pass trails and weather swings matter), and training smart.
Stop treating symptoms. Start fixing the system.
And if you’re ready to stop being sidelined by pain and get back to the activities you love— without fear of the ache returning—then you’re in the right place. At WYNOT Fitness, we build movement systems that match your life, your terrain, your weather, and your goals. Be WYNOT Strong.
Contact info@wynotfit.com with any questions you may have.




Thank you for the article and the 8 Free Exercise Guide. I have been fighting knee pain and finally figured out what it was. Thank you WYNOT Fitness.